Non-Small Cell Lung Cancer
Non-small cell lung cancer is the most common form of lung cancer tumors. The major cause is smoking followed by asbestos and other pollutants.
Non-Small Cell Lung Cancer Facts
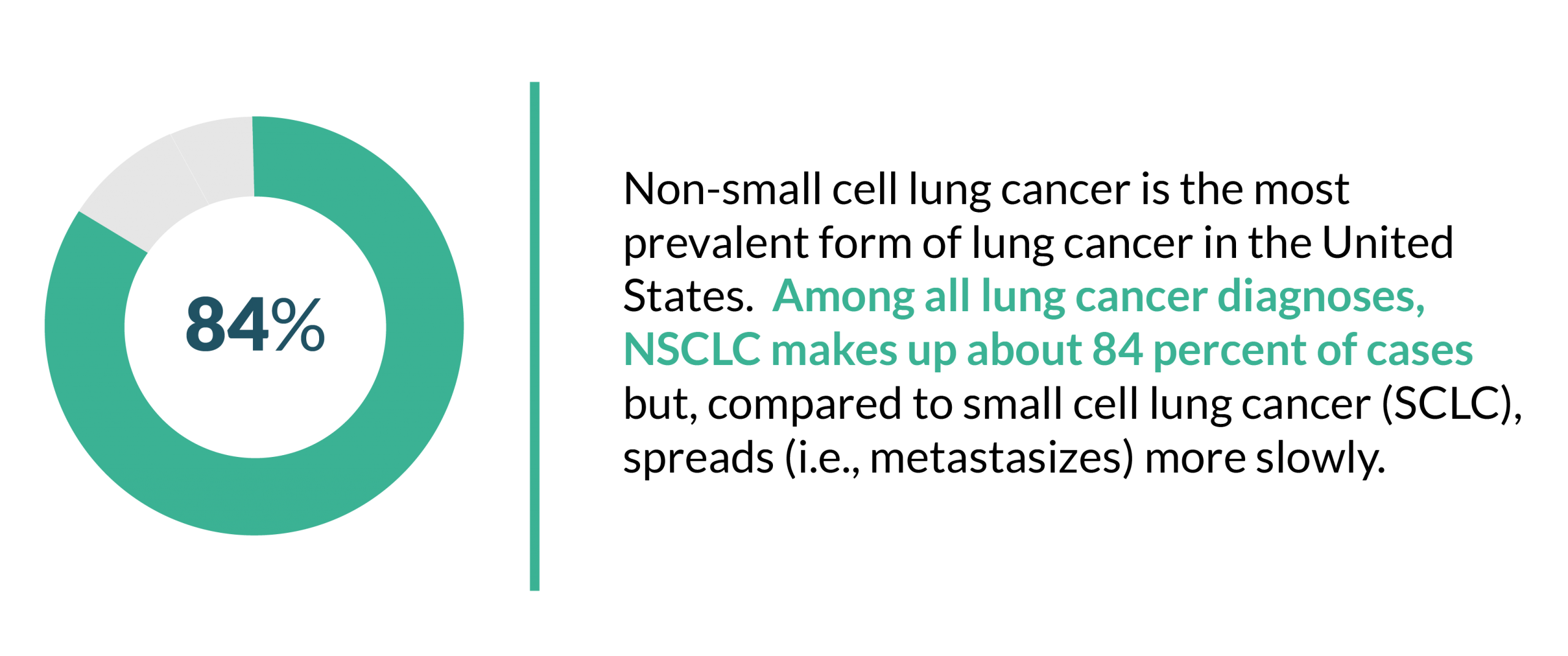
Non-small cell lung cancer is the most prevalent form of lung cancer in the United States. (NSCLC) Among all lung cancer diagnoses, NSCLC makes up about 84 percent of cases but, compared to small cell lung cancer (SCLC), spreads (i.e., metastasizes) more slowly. As such, common NSCLC symptoms usually involve a chronic cough and shortness of breath. While early screenings, physical exams, and imaging tests help detect the presence of lung cancer, a biopsy is needed to diagnose NSCLC.
Beginning in the lung tissue, NSCLC has three subtypes: adenocarcinoma, large cell carcinoma, and squamous cell carcinoma. Each subtype is defined by the appearance of its cancer cells under a microscope. Though each type is generally found in a specific area of the lung, a biopsy (i.e., analysis of a cell sample via extraction with a needle) is used to help doctors diagnose the type and stage of cancer.
Typically, the prognosis for NSCLC depends on a variety of factors including the stage of cancer and the patient’s overall health. Fortunately, NSCLC can be cured if caught early. However, according to the National Cancer Institute, most patients with NSCLC today have advanced cancer that is not curable with modern techniques.
NSCLC Symptoms
For most people, signs of non-small cell lung cancer begin with a persistent cough, shortness of breath, and some chest pain. In many cases, however, early NSCLC does not cause any symptoms. Symptoms that often become noticeable or worsen in advanced stages of the illness include:
- Bone pain
- Coughing up blood
- Eyelid drooping
- Hoarse voice
- Fatigue
- Joint pain
- Loss of appetite
- Nail problems
- Swelling of the face
- Unexplained weight loss
- Weakness
- Wheezing
At times, these symptoms may cause doctors to misdiagnose NSCLC as pneumonia, tuberculosis, or other respiratory illness. This is often due to overlapping risk factors and causes of lung diseases. For instance, smoking cigarettes, radon, asbestos exposure, diesel exhaust inhalation, and pollution can increase a person’s risk for simple respiratory illnesses like bronchitis as well as malignant cancers like NSCLC and mesothelioma.
Testing and Diagnosis
To confirm the presence of lung cancer, tests such as bone, CT, and PET scans; chest x-rays, MRIs, and sputum analyses are commonly prescribed. To diagnose non-small cell lung cancer, a biopsy of the tumors is the next step. Also, biopsies can be combined with other tests or procedures to more accurately stage the patient’s NSCLC. These combinations include:
- Bronchoscopy with biopsy
- CT-scan-directed needle biopsy
- Endoscopic esophageal ultrasound (EUS) with biopsy
- Mediastinoscopy with biopsy
- Open lung biopsy
After a biopsy, NSCLC patients are likely to be diagnosed with one of the following subtypes of the disease.
- Adenocarcinoma: Usually located in the outer lung in sacs that make fluids like mucus; most common form.
- Squamous carcinoma: Usually located in the center of the lung next to bronchi; makes up about 25 percent of cases.
- Large cell (undifferentiated) carcinoma: Located in any part of the lung. Metastasizes quickly and makes up about 10 percent of cases.
Other, less common NSCLC subtypes include adenosquamous carcinoma and sarcomatoid carcinoma.
Staging and Prognosis
Using the information from imaging tests and biopsies, doctors stage NSCLC between zero and IV – with higher numbers indicating greater levels of metastasis.
Stage |
Description |
| Stage 0 | Cancerous cells present in the lining of one area of a lung. |
| Stage I | Tumors contained to a single area in the lung with no spread to lymph nodes. |
| Stage II | Cancer has reached nearby lymph nodes next to the primary tumor. |
| Stage III | Cancer is affecting neighboring tissues and distant lymph nodes. |
| Stage IV | Cancer has metastasized to additional organs, traveling via the bloodstream to the brain or liver. |
Similar in its description of tumor spread, the American Joint Committee for Cancer Staging and End Results Reporting uses the TNM system (size of primary Tumor, spread to lymph Nodes, and the extent of Metastasis) for many lung cancers and was updated for NSCLC in 2010. Further categorization within the system exists to classify prognoses.
The prognosis for NSCLC varies depending on the age, health of the patient, and stage of the disease. Compared to other forms of lung cancer, NSCLC spreads more slowly, giving patients the opportunity to catch and treat it early. Yet, some cases of NSCLC can be aggressive and fatal in a relatively short period of time.
Overall, Stages I and II have the best prognosis, highest survival rates, and the best odds of receiving curative treatment. Meanwhile, Stage III is curable only in some cases and Stage IV has little chance of ever receiving a cure. Most Stage IV patients are given palliative treatment with the goal of easing pain. The localized NSCLC five-year survival rate is 61 percent (meaning 61 percent of patients with localized NSCLC have survived at least five years after their initial diagnosis); the five-year survival rate for regional NSCLC is 35 percent. If tumors have reached other organs and distant lymph nodes, the five-year survival rate falls to just six percent.
Treatment
The treatment of non-small cell lung cancer depends heavily on the stage at which the patient was diagnosed. Early-stage NSCLC responds well to chemotherapy; primary tumors may also be removed via surgery. Subsequently, chemotherapy, surgery, and radiation are the most common treatment options and are usually prescribed in some combination to provide the most therapeutic value.
Stage I and II tumors are typically removed through inpatient or outpatient surgery (commonly referred to as resection). Lobectomy (removal of a lung section), pneumonectomy (removal of a whole lung), and wedge resection (removing a section of a lobe) are the most common procedures.
Due to its adjuvant and neoadjuvant use, chemotherapy is used on up to 80 percent of all lung cancer patients. First-line chemotherapy, according to the American Society for Clinical Oncology (ASCO), should involve a platinum combination. Cisplatin and carboplatin are the most common chemotherapy medications prescribed to NSCLC patients.
Of the three, radiation therapy alone is the least common form of treatment. If NSCLC tumors are not removable via surgery, radiation is used. For patients who are unable to undergo or recover from surgery, stereotactic radiation is the most viable treatment option.


